

| FAQ/Help |
| Calendar |
| Search |
| Today's Posts |
 01-28-2007, 02:52 PM
01-28-2007, 02:52 PM
|
#1 | |||
|
||||
|
In Remembrance

|
We are flooding GregD's thread with the BBB posts so I thought I would open a separate thread, so as not to hijack his. All are welcome to put as much information as we can find on the link between BBB porosity and PD and other neurological diseases.
In GregD's thread, I gave evidence that Parkies all show disruption of the BBB, (Prof Leenders in Holland) and that a process or treatment like stress increases the porosity of the BBB and makes symptoms worse, whilst a tightening of the BBB with for example curcumin, improves symptoms. One report I found states, "Alzheimers disease may be due to a breakdown in the blood brain barrier." http://en.wikipedia.org/wiki/Blood-brain_barrier Alzheimers Disease New evidence indicates that disrupton of the blood brain barrier in AD patients allows beta amyloid containing blood plasma to enter the brain where the A beta adheres perferentially to the surface of astrocytes. These findings have led to hypothesize that (1) breakdown of the blood-brain barrier allows access of neuron-binding autoantibodies and soluble exogenous Aβ42 to brain neurons and (2) binding of these autoantibodies to neurons triggers and/or facilitates the internalization and accumulation of cell surface-bound Aβ42 in vulnerable neurons through their natural tendency to clear surface-bound autoantibodies via endocytosis. Eventually the astrocyte is overwhelmed, dies, ruptures, and disintegrates, leaving behind the insoluble Aβ42 plaque. Thus Alzheimers disease may be due to a breakdown in the blood brain barrier. [4] Another report cites damage to the BBB is the cause of MS. http://en.wikipedia.org/wiki/Blood-brain_barrier "stabilization of the blood-brain barrier integrity Some diseases, such as MS, begin with the BBB breakdown" In the report below,it suggests that " Wouldn't repairing the blood-brain barrier help to "cure" MS? http://serendip.brynmawr.edu/bb/neur...3/Johnson.html " Earlier studies have revealed the relative permeability of the molecule (MTPT), through the blood-brain barrier and its ability to induce Parkinson-like symptoms in rats." http://209.85.165.104/search?q=cache...k&ct=clnk&cd=3 So what determines who gets Alzheimers, who gets MS and who gets PD? Is one section damaged which gives PD whilst another gives AZ? Does a damaged section of the BBB admit a compound which causes MS, whilst another damaged section causes PD by admiting a different toxin. Is it related to time scale in how long the BBB has been "leaky", ie a very long history of low porosity leakage,l letting in small molecule toxins may give PD, whilst a short term major damage may open the floodgates and admit larger molecules which can cause AZ. It matters whether the compound has an electrical charge, and the size of the molecule. There does seem to be a strong link between the BBB permeability and neurological disease. Can we find other evidence on what effect a compound or treatment has on the porosity of the BBB, and what is it's effect on PD. The final goal will be to find a treatment which closes the BBB long term and effectively cures PD. Lets start searching. Ron |
|||

|
 Reply With Quote Reply With Quote
|
|
01-28-2007, 05:18 PM
|
#2 | |||
|
||||
|
In Remembrance

|
....whether it be meditation, exercise, prayer, hypnosis, massage, etc.
1: Front Biosci. 2007 Jan 1;12:1615-28. Corticotropin-releasing hormone and the blood-brain-barrier. Theoharides TC, Konstantinidou AD. Department of Pharmacology and Experimental Therapeutics, Tufts University School of Medicine and Tufts-New England Medical Center, 136 Harrison Avenue, Boston, MA 02111, USA. theoharis.theoharides@tufts.edu Increased blood-brain-barrier (BBB) permeability precedes any clinical or pathologic signs and is critical in the pathogenesis of multiple sclerosis (MS) and brain metastases. CD4+ TH1 cells mediate demyelination in MS, but how they get sensitized and enter the brain to induce brain inflammation remains obscure. TH2 cytokines associated with allergic disorders have recently been implicated in MS, while genes upregulated in MS plaques include the mast cell-specific tryptase, the IgE receptor (Fc-epsilon-RI) and the histamine-1 receptor. Mast cell specific tryptase is elevated in the CSF of MS patients, induces microvascular leakage and stimulates protease-activated receptors (PAR), leading to widespread inflammation. BBB permeability, MS and brain metastases appear to worsen in response to acute stress that leads to the local release of corticotropin-releasing hormone (CRH), which activates brain mast cells to selectively release IL-6, IL-8 and vascular endothelial growth factor (VEGF). Acute stress increases BBB permeability that is dependent on CRH and mast cells. Acute stress shortens the time of onset of experimental alleric encephalomyelitis (EAE) that does not develop in W/W mast cell deficient or CRH -/- mice. Brain mast cell inhibition and CRHR antagonists offer novel therapeutic possibilities. PMID: 17127408 [PubMed - in process]
__________________
Born in 1953, 1st symptoms and misdiagnosed as essential tremor in 1992. Dx with PD in 2000. Currently (2011) taking 200/50 Sinemet CR 8 times a day + 10/100 Sinemet 3 times a day. Functional 90% of waking day but fragile. Failure at exercise but still trying. Constantly experimenting. Beta blocker and ACE inhibitor at present. Currently (01/2013) taking ldopa/carbadopa 200/50 CR six times a day + 10/100 form 3 times daily. Functional 90% of day. Update 04/2013: L/C 200/50 8x; Beta Blocker; ACE Inhib; Ginger; Turmeric; Creatine; Magnesium; Potassium. Doing well. |
|||
|
|
Reply With Quote
|
|
01-28-2007, 05:46 PM
|
#3 | |||
|
||||
|
In Remembrance
|
Looking at that abstract that I just put up made me realize that I have over immersed myself in all this of late and that a good number of those who need the info won't understand that mess. So let me give the two cent summary and then a link to one of the handiest tools I have ever found.
"Acute stress increases BBB permeability that is dependent on CRH and mast cells." That's the part that applies to our discussion. CRH is corticotropin-releasing hormone which is what your brain squirts out to start the process of the "fight or flight" response. The rest is not relevant to us so don't stress yourself over it.  Now, the tool is called "1-Click Answers" and is a work of art. You download it, install, and forget all about it. But anytime, anywhere you encounter a word or phrase that's unfamiliar - just "Alt-Click" on it and a dandy little window pops up and gives you the definition. It sure helps with these papers. http://www.answers.com/main/home_simple.jsp -Rick
__________________
Born in 1953, 1st symptoms and misdiagnosed as essential tremor in 1992. Dx with PD in 2000. Currently (2011) taking 200/50 Sinemet CR 8 times a day + 10/100 Sinemet 3 times a day. Functional 90% of waking day but fragile. Failure at exercise but still trying. Constantly experimenting. Beta blocker and ACE inhibitor at present. Currently (01/2013) taking ldopa/carbadopa 200/50 CR six times a day + 10/100 form 3 times daily. Functional 90% of day. Update 04/2013: L/C 200/50 8x; Beta Blocker; ACE Inhib; Ginger; Turmeric; Creatine; Magnesium; Potassium. Doing well. |
|||
|
|
Reply With Quote
|
|
01-28-2007, 05:48 PM
|
#4 | ||
|
|||
|
In Remembrance
|
Ron said: Is it related to time scale in how long the BBB has been "leaky", ie a very long history of low porosity leakage,l letting in small molecule toxins may give PD, whilst a short term major damage may open the floodgates and admit larger molecules which can cause AZ. It matters whether the compound has an electrical charge, and the size of the molecule.
Is it feasible to think that at any time the "damn could burst" a nd even if just some, not all of it leaks, that could represent the "big drop" that many neuros have warned us about at diagnosis. Well I guess we have our own little ozone layers. Can you please explain: "depends on whether the compound has an electrical charge?' thank you, paula
__________________
paula "Time is not neutral for those who have pd or for those who will get it." |
||
|
|
Reply With Quote
|
|
01-28-2007, 06:27 PM
|
#5 | ||
|
|||
|
Member
|
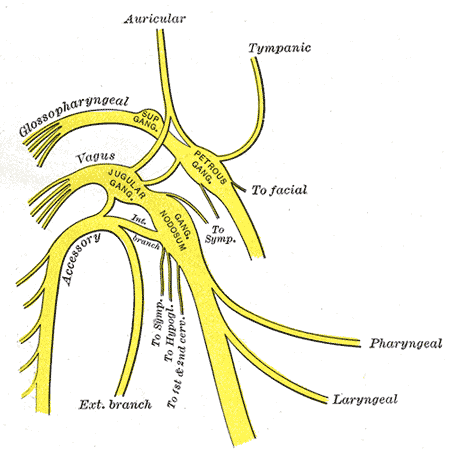 While trying to put 2 and 2 together and come up with 4 I stumbled onto something that I find very interesting and, yes, exciting. I was reviewing in my mind all of the myriad symptoms that tend to pop up in our bodies at times that don't seem to be included in the description of the Parkinson's model (i.e. tremor, poverty of movement, gait, etc). Some of these include problems with speech, swallowing, acid reflux, ringing in the ears, visual halucinations, weight fluctuation, excessive sweating, breathing, etc. What one mechanism or structure in our body can tie all of these areas together and provide access to the Substantia Nigra through the Blood Brain Barrier. The answer was there, staring me in the face. The Vagus Nerve (pictured above) is involved in absolutely every one of these problems. So could it be that the Vagus Nerve suffers inflammation which causes a leaky seal at the BBB and allows any number of substances to not only penetrate th;e BBB but penetrate it at the point at which neurotoxins would have to go in order to affect Parkinson's disease. http://en.wikipedia.org/wiki/Vagus_nerve Quote:
http://www.jneurosci.org/cgi/reprint/5/6/1387.pdf Quote:
Last edited by michael7733; 01-28-2007 at 06:51 PM. |
||
|
|
Reply With Quote
|
|
01-28-2007, 07:02 PM
|
#6 | |||
|
||||
|
In Remembrance
|
<Begin Quote>
The Vagus Nerve (pictured above) is involved in absolutely every one of these problems. So could it be that the Vagus Nerve suffers inflammation which causes a leaky seal at the BBB and allows any number of substances to not only penetrate th;e BBB but penetrate it at the point at which neurotoxins would have to go in order to affect Parkinson's disease. I will be editing this in a few minutes to include some documentation.<End Quote> There is a German scientist named Braak that within the last ten years has been pointing some very interesting things involving, among other things, the vagus nerve. There are little knots of protein found in the neurons of PWP and they are called Lewy bodies after the guy who found them. All that is really known about them is that they are always found in the substantia nigra of deceased PWP. In fact, they are the "gold standard" for defining PD. What Braak noticed was that the Lewy bodies (LB) actually showed up in other areas of the nervous system *years* before they made it to the SN. In fact the first places they show up are the olfactory bulb of the nose and an area in the stomach wall. Then they spread, step by step and from two directions, into the brain and eventually show up in the SN and our problems begin. Our bodies actually have a transport system along our nervefibers and it goes in both directions. The route taken from the nose is along the fibers that conduct the sense of smell. The route from the lower regions is, you guessed it, the vagus nerve. So here we have another possible hole in the BBB defences. And something moves along the fibers that pass through that hole leaving a trail of LBs behind. Toxin? Virus? Pesticide? My own bet is the toxins like those put out by our old friend H pylori. But there is no reason to assume that is is just one or the other. Maybe that is part of why we vary so much is speed of progression.
__________________
Born in 1953, 1st symptoms and misdiagnosed as essential tremor in 1992. Dx with PD in 2000. Currently (2011) taking 200/50 Sinemet CR 8 times a day + 10/100 Sinemet 3 times a day. Functional 90% of waking day but fragile. Failure at exercise but still trying. Constantly experimenting. Beta blocker and ACE inhibitor at present. Currently (01/2013) taking ldopa/carbadopa 200/50 CR six times a day + 10/100 form 3 times daily. Functional 90% of day. Update 04/2013: L/C 200/50 8x; Beta Blocker; ACE Inhib; Ginger; Turmeric; Creatine; Magnesium; Potassium. Doing well. |
|||
|
|
Reply With Quote
|
|
01-28-2007, 08:37 PM
|
#7 | ||
|
|||
|
New Member
|
Very interesting hypothesis - definately could use some investigation
Having been on Sodium Warfarin (Coumadin) for over a year following a severe head trauma I am beginning to wonder if there is a causality link. And the formation of Lewy Bodies in the neurons in response even makes the link more plausable. Warm Regards from Arizona, Ralph :-) |
||
|
|
Reply With Quote
|
|
01-29-2007, 01:33 AM
|
#8 | |||
|
||||
|
In Remembrance
|
Paula,
Quote,"Can you please explain: "depends on whether the compound has an electrical charge?'" There is an explanation below, but I would read it then forget it!! I was only trying to think of how many ways a toxin entering the brain could differ, in order to explain why we get one illness or another. A molecule is neutral, and has no electric charge. When a molecule can split into 2 parts, and one part takes the electrons they share forming a bond, it means the part which lost the electrons is positively charged, whilst the part which gained the electrons is negatively charged. So in magnesium chloride, MgCl2, it goes to Mg++ and Cl--. The Mg++, the magnesium ion is positively gharged and the chlorine ion Cl-- is negatively charged. Contrast this with say a toxic benzene molecule, C6H6, which is a neutral molecule, and does not split into charged parts called ions. The gap in the BBB could have a charge or not, and it would affect what it admitted. I was over complicating things by adding in the possibility of whether the toxin could have a charge. Ron |
|||
|
|
Reply With Quote
|
|
01-29-2007, 04:49 AM
|
#9 | |||
|
||||
|
In Remembrance
|
In 1918, there was an epidemic/pandemic (not sure of the difference), but a lot of people got encephalitis. They later all developed PD. Why?
Because encephalitis causes the BBB to widen its pores. "Viruses are another possible environmental trigger for PD. People who developed encephalopathy after a 1918 influenza epidemic were later stricken with severe, progressive Parkinson's-like symptoms." http://www.ninds.nih.gov/disorders/p...ns_disease.htm Just editing this to add that whilst the BBB is there to keep out certain molecules, it also stops a number of drugs that the medics want to use on PD. To get these drugs in to the brain, they either use a "trojan horse" method, or they deliberately open the pores of the BBB with a compound that widens the pores, and add the drug. In the above report on encephalitis, the BBB is only open for the duration of the disease. This pushes forward the day they reach the threshold of 80% of neurons put out of action, and PD starts. So are the medical people piling up problems for their patients by temporarily opening the BBB to let their drugs in, plus a rush of toxins that cause the person to get PD at some later date??? Ron Last edited by Ronhutton; 01-29-2007 at 06:59 AM. |
|||
|
|
Reply With Quote
|
|
01-29-2007, 09:51 AM
|
#10 | |||
|
||||
|
In Remembrance
|
I have been taking CDP Choline (also called citicholine) now (250mg to 500mg per day), along with my curcumin for 5 years. I recommended the two supplements a number of times on the old MGH site.
I have now found that not only curcumin reduces the permeability of the BBB, but so does citicholine. A good review of citicholine is at Citicoline: The Brain Protecting Choline Supplement http://www.naturalproductsinsider.co...ngredient.html I took citicholine since it is given to stroke victims in the UK, and is said to assist brain metabolism. I did not know it also had a beneficial effect on the BBB. One bit of bad news, I don't think it is approved in the USA. Ron |
|||
|
|
Reply With Quote
|
| Reply |
|
|
 Similar Threads
Similar Threads
|
||||
| Thread | Forum | |||
| The Blood Brain Barrier | Parkinson's Disease | |||
 Linear Mode
Linear Mode

